
By Brandy Ramaj Jewett, DAT, LAT, ATC
It has been estimated that 63 percent of individuals participating in sports will suffer a spondylolysis and 6 to 8 percent of individuals suffering low back pain (LBP) are diagnosed with a spondylolithesis.1 Additionally, there are few preclinical indications unique to spondylosis.1,2 This leads many authors to believe the condition is often underdiagnosed.1
If left untreated, spondylolysis can progress to a bilateral pars interarticularis defect known as spondylolisthesis, which can lead to an increased risk of dysfunction and inability to participate in sport.3 Accurate diagnosis is crucial in initiating proper treatment for spondylolysis to prevent progression to spondylolisthesis and increased risk of dysfunction. Computed tomography (CT) is considered the gold standard for assessing body defects of the pars interarticularis but exposes the patient to high levels of radiation and can be costly to patients.4 Therefore, the utilization of accurate clinical tests is crucial when determining whether advanced imaging is warranted in patients suspected of a spondylolysis.
Symptoms of pars interarticularis defects are similar to other lumbar pathologies causing challenges in determining whether advanced imaging techniques are warranted.3 Commonly patient history data, the standing stork test and spring test are used to diagnose. However, clinicians should be aware of the accuracy and clinical utility of special tests and patient history data in guiding clinical decision-making in patients with LBP suspected of suffering spondylolysis or spondylolisthesis.
Clinical Question
In patients with LBP, which exam findings are the most accurate in diagnosing lumbar spondylolysis and spondylolisthesis?
Summary of Findings
A literature search of Medline, CINHAL and SportDiscus returned two systematic reviews1,5 that investigated diagnostic accuracy of subjective and objective exam findings in the clinical diagnosis of spondylolysis and spondylolisthesis. A 2016 review5 is an update of a similar systemic review1 published in 2014 with the addition of two clinical tests, the evaluation of patient history data and narrowed inclusion criteria to studies investigating athletes younger than 20 years of age suffering LBP.
Additionally, three systematic reviews were found investigating the diagnostic value of magnetic resonance imaging in diagnosing spondylolysis and spondylolisthesis.2,6,7 CT is currently the gold standard for diagnosing defects of the pars interarticularis.2,4,6 However, concerns related to ionizing radiation exposure for young patients warrants discussion of the diagnostic accuracy of an alternative imaging techniques.
Spondylolysis
Patient History Data. The 2016 systematic review5 identified five patient data history variables used to diagnose spondylolysis. Age at evaluation, gender, duration of symptoms less than three months, sudden onset of symptoms and participation in sport were assessed.5 Sudden onset of symptoms (sensitivity=88 percent, specificity=51 percent) and sports participation (sensitivity=85 percent, specificity=34 percent) had the highest diagnostic value for spondylolysis.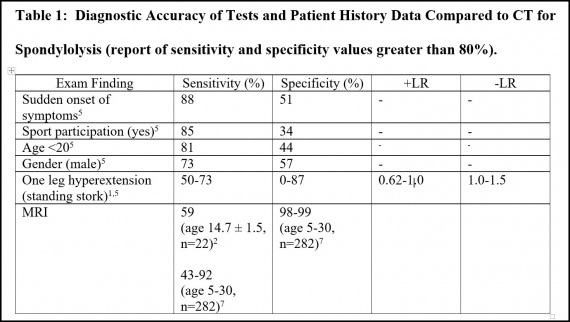
Special Tests and Exam Findings. Of the 34 clinical tests,1,5 single leg hyperextension was documented to have the highest sensitivity (50 to 73 percent) and specificity (zero to 87 percent) in diagnosing spondylolysis.5 However, the authors discussed the sensitivity and specificity values were not high enough to consider this test reliable in clinically diagnosing spondylolysis. Other clinical findings evaluated were hamstring contraction, lumbar range of motion (ROM), single leg raise, double leg raise, femoral nerve stretch, Achilles and patellar reflexes and loss of ankle and great toe extension strength.5 While tests such as hamstring contraction, lumbar extension, double leg raise and loss of ankle and great toe extension strength had high specificity values (ranging 80 to 100 percent) all of the aforementioned tests had low sensitivity values and therefore aren’t considered reliable in the diagnosis of spondylolysis in young patients with LBP.5
Spondylolisthesis
Patient History Data. Of the 19 patient history data variables assessed, three had sensitivity values greater than 80 percent: “pain worse with sitting” (sensitivity=85 percent), “wake up from sleep due to pain” (sensitivity=81 percent) and “pain worse with walking” (sensitivity=80 percent).5 Pain in the gluteal region had the highest specificity at 96 percent (sensitivity=16 percent). Interestingly, localized LBP showed poor diagnostic value (sensitivity=23 percent; specificity=77 percent).5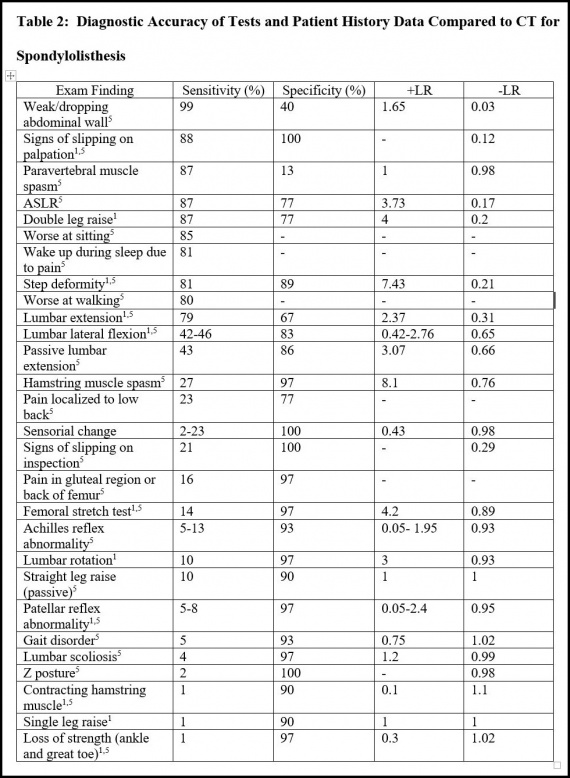
Special Tests and Exam Findings. Several physical exam findings were reported in the 2015 and 2016 systematic reviews for the clinical diagnosis of spondylolisthesis.1,5 Sign of vertebral slipping upon palpation (sensitivity=88 percent; specificity=100 percent), active straight leg raise (sensitivity=87 percent; specificity=77 percent), double leg raise (sensitivity=87 percent; specificity=77 percent) and step deformity (sensitivity=81 percent; specificity=89 percent) showed the most diagnostic value. Lumbar ROM (extension, flexion, rotation, lateral flexion and passive extension) had sensitivities ranging 10 to 79 percent and specificities ranging 67 to 97 percent.
Clinical Imaging Techniques
Of the three reviews investigating advanced clinical imaging techniques, a 2015 review6 reported CT outperforms radiograph in diagnosing spondylolysis at comparable doses of ionizing radiation among children and young adults (ages 5 to 18). CT was reported to have increased agreement between raters, with the Kappa for rater agreement of radiographs ranging 0.24 to 0.4 and a Kappa of 0.88 for rater agreement with CT.6 The average radiation effective dose from lumbar radiography was reported at 0.209 for a single view image, while the effective dose from a single CT is 0.4.6 It is important to note, lumbar radiographs are typically ordered in four views when diagnosing a pars defect (AP, oblique, lateral and spot). Therefore, the combined effective dose from the standard views for spondylolysis radiographs is estimated to be more than that of a single CT.6 This finding suggests the common use of radiographs in the diagnosis of pars defects is unnecessarily exposing patients to ionizing radiation as most patients will require a CT in addition to the radiograph for more accurate diagnosis.6
A 2017 review7 revealed the use of MRI to be comparable to the gold standard CT among children and young adults (ages 5 to 30, n=282). When measured against CT, sensitivity and specificity values for MRI in children and young adults were on average 81 percent and 99 percent, respectively.7 The authors considered the high clinical value of MRI and suggested MRI be first choice in diagnosing a spondylolysis or spondylolisthesis, especially in young children. However, a recent 2019 cross-sectional study2 challenges this by revealing CT to be significantly more accurate than MRI in diagnosing spondylolysis.
The 2019 study examined 22 children and adolescents (ages 13 to 16) suspected of a pars defect (with no control group). All participants were examined with both MRI and CT scans on the same day.2 In this study, MRI was found to have a lower sensitivity of 58.1 percent than presented by the 2017 review.2 While the 2019 study demonstrated CT to be superior to MRI, the authors discussed MRI may still be a better diagnostic tool in evaluating children and young adults with LBP as MRI is shown to be superior in diagnosing differential diagnoses such as disc pathology, stenosis and nerve root pathology.2 Additionally, MRI doesn’t expose the patient to ionizing radiation2 and has clinical value in the diagnosis of pars interarticularis defects.7
Clinical Bottom Line
Spondylolisthesis
A detailed history on pain patterns and symptoms may prove valuable in the clinical diagnosis of a bilateral parts defect. Details about sleep disruptions and positional pain patterns (sitting, walking) have moderate diagnostic values. When these patient history data variables are combined with commonly used objective findings such as step deformity, vertebral slipping, double leg raise and lumbar ROM, spondylolisthesis can be more accurately diagnosed clinical compared to a unilateral pars defect.
Spondylolysis
Current clinical diagnostic practices are more accurate in ruling out a spondylolysis verses ruling in the condition. If a patient isn’t participating in a sport, isn’t a male younger than 20, doesn’t report a sudden onset of symptoms and doesn’t present with a positive single leg hyperextension test, a clinician can be moderately certain the patient doesn’t have a spondylolysis defect. Therefore, this patient should be treated conservatively and monitored for progression or resolution of symptoms. If the patient does participate in a sport, is a male younger than 20, reports a sudden onset of symptoms and tests positive for pain during the single leg hyperextension test, the clinician should consider diagnostic imaging for more accurate diagnosis.
In patients younger than 18, MRI should be considered as the preferred study as MRI has been shown to have high diagnostic value and prevents exposure to ionizing radiation.7 Additionally, patients who do not satisfy all aforementioned clinical diagnosis criteria for a pars defect may be suffering a differential diagnosis of which MRI is considered superior in diagnosing. However, MRI may be more likely to present a false-negative result for a pars defect.2 Therefore, patients older than 18 may consider CT be performed to diagnosis a spondylolysis with less likelihood of a false-negative finding.
Furthermore, CT and MRI should be considered over radiograph in the diagnosis of spondylolysis or spondylolisthesis as this tool is shown to have more false-negative findings of the three imaging studies and exposes the patient to comparable ionizing radiation levels as CT.6
Future Directions
Further research and development of more accurate clinical decision-making guidelines are needed to guide accurate diagnosis of spondylolysis before the condition progresses to spondylolisthesis. Likely, combinations of the tests and clinical findings noted in this report could increase diagnostic values thereby improving clinical decision-making. Future research should investigate the validity of such combinations.
References
1. Alqarni AM, Schneiders AG, Cook CE, Hendrick PA. Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic review. Physical Therapy in Sport. 2015;16(3):268-275. doi:10.1016/j.ptsp.2014.12.005
2. West AM, d’Hemecourt PA, Bono OJ, Micheli LJ, Sugimoto D. Diagnostic Accuracy of Magnetic Resonance Imaging and Computed Tomography Scan in Young Athletes With Spondylolysis. Clin Pediatr (Phila). 2019;58(6):671-676. doi:10.1177/0009922819832643
3. Shah SA, Saller J. Evaluation and Diagnosis of Back Pain in Children and Adolescents: Journal of the American Academy of Orthopaedic Surgeons. 2016;24(1):37-45. doi:10.5435/JAAOS-D-14-00130
4. Ledonio CGT, Burton DC, Crawford CH, et al. Current Evidence Regarding Diagnostic Imaging Methods for Pediatric Lumbar Spondylolysis: A Report From the Scoliosis Research Society Evidence-Based Medicine Committee. Spine Deformity. 2017;5(2):97-101. doi:10.1016/j.jspd.2016.10.006
5. Grødahl LHJ, Fawcett L, Nazareth M, et al. Diagnostic utility of patient history and physical examination data to detect spondylolysis and spondylolisthesis in athletes with low back pain: A systematic review. Manual Therapy. 2016;24:7-17. doi:10.1016/j.math.2016.03.011
6. Fadell MF, Gralla J, Bercha I, et al. CT outperforms radiographs at a comparable radiation dose in the assessment for spondylolysis. Pediatr Radiol. 2015;45(7):1026-1030. doi:10.1007/s00247-015-3278-z
7. Dhouib A, Tabard-Fougere A, Hanquinet S, Dayer R. Diagnostic accuracy of MR imaging for direct visualization of lumbar pars defect in children and young adults: a systematic review and meta-analysis. Eur Spine J. 2018;27(5):1058-1066. doi:10.1007/s00586-017-5305-2




