
By Dana Bates, PhD, LAT, ATC, and Jessica Moore, EdD, LAT, ATC
Clinical education for athletic training students was suddenly questionable for some programs and came to a standstill for others when the COVID-19 pandemic began its first nationwide toll in the U.S. in March 2020. As such, athletic training programs were faced with the ongoing challenge of cultivating athletic training student skill development in preparation for professional practice. While supplemental clinical experiences such as simulation and/or telemedicine and telehealth were acceptable to meet educational requirements and on-time graduation1,3, athletic training programs remained obligated to teach and assess curricular content standards and require clinical education while preparing future athletic trainers to be safe and effective health care providers.
Clinical education and patient interaction are important parts of students’ education and many clinical education coordinators may be struggling to find or replace experiences that still challenge athletic training students similar to immediate care and participation in practices and events during the pandemic. For much of the U.S., fall 2020 continued to challenge programs’ ability to place students in clinical educational experiences.
As our clinical education team at Pacific University met to discuss moving forward with clinical education, we began to investigate alternative strategies that would enable students to utilize skills through direct patient-care opportunities, rather than only creating guided simulation experiences. As a solution, our program transitioned our teaching lab into an operating clinic during the COVID-19 pandemic to provide valuable hands-on athletic training experiences for students. For those programs looking to create patient care opportunities, figure 1 provides a list of key considerations.
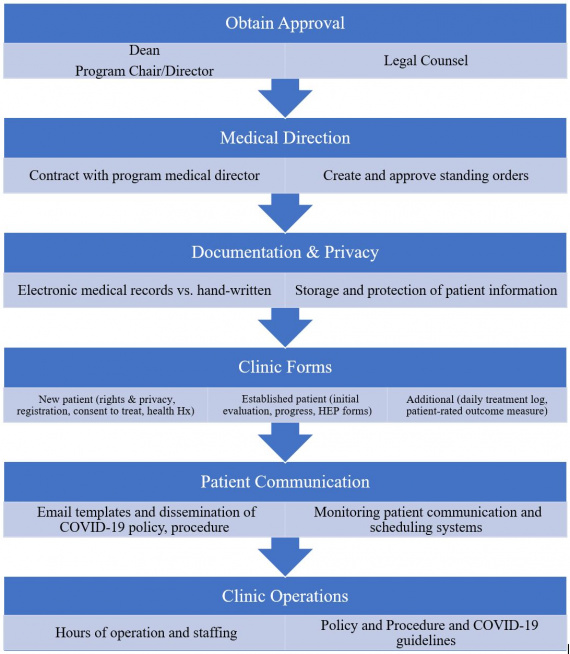
During the current pandemic, programs must consider all necessary approvals to create a functional clinic on campus. These may be specific institutional COVID-19 tasks forces, college and school directors and deans and legal counsel. Consideration of financial costs, physical space, accessing patients, patient safety and any Centers for Disease Control and Prevention (CDC), state and/or regional mandates.
At Pacific University, our program is housed in the College of Health Professions, where several clinics already function. As such, we had successful models to follow and the process of approval was relatively quick.
Athletic trainers work under the direction of or in collaboration with a supervising physician. All accredited athletic training programs have a medical director, who can be a valuable advocate for creating a clinic and naturally fill the role of supervising physician. In developing our clinic, we worked with our medical director to enter into an agreement to serve as our supervisory physician and create standing orders. These standing orders emphasized musculoskeletal evaluation, treatment and rehabilitation to include electrical and manual therapies, supportive techniques, such as taping and bracing, functional testing and ongoing evaluation as deemed necessary and appropriate. University faculty would serve as preceptors. The emphasis on musculoskeletal conditions was purposeful since we would not see injuries associated with trauma or bleeding, therefore our standing orders did not include skills and procedures associated with emergency care.
Consideration of space and available equipment to evaluate and treat patients is important, especially when following CDC, state and/or regional guidelines for appropriate spacing needs for safe patient care. Our program has a dedicated teaching lab space of about 1,600-square-feet with 10 treatment tables, a treadmill, bike, various therapeutic modalities (e.g., ice packs, moist heat packs, paraffin, electrical stimulation and ultrasound, portable TENS units and cold pneumatic compression) and rehabilitation equipment (e.g., elastic bands, hand-held and cuff weights, foam rollers, BOSU balance pads, Theraballs, squat rack and weights). Our teaching lab space and the presence of equipment already used for educational purposes was ideal for transitioning into an active clinical site. While we had access to the equipment listed, opening an active clinic in teaching spaces can be successful with creativity and use of equipment you may already have available.
When discussing clinic hours of operation, we identified an afternoon schedule that would best fit our students' needs as classes would be complete by the afternoon.
As programs prepare future health care providers, one content area often cited as a weakness is administration.4,5 When developing a clinic, there are many policies and procedures, clinic documents and forms, and now COVID-19 screening protocols that must be created. Assigning these administrative tasks to students supports active practice and experience with creating and implementing administrative tasks that may not occur often during students’ traditional athletic training experiences. The students in our program had very little previous administrative experience, therefore it was a great opportunity for them to create new documents and templates and build a policy and procedure manual from the ground up. Our first-year cohort was actively involved in this administration piece as well, collaborating, reviewing and creating missing parts of the policy and procedure manual.
|
Sample Clinic Policy and Procedures |
|
As a faculty, we served as preceptors and felt strongly about pushing students to take ownership of the clinic, thereby leaving a lot of the decision-making to them, which included mission and vision, patient confidentiality, code of conduct and professionalism, emergency action plan, and policies regarding clinic operations. This proved to be valuable, enabling them to feel ownership of and buy into the clinic, offering students an experience different from other clinical sites that may have followed a more hierarchical management style.
It is also important to consider electronic medical records (EMR) program and means of documentation when developing a clinic. When considering best documentation practices, also consider costs. Due to our program not having any funding for an EMR program, we elected to use paper documentation. While CAATE standards emphasize use of electronic health records to document health-related information, we found that returning to hand-written documentation further created teachable moments and underlined the importance of appropriate medical charting and documentation for our students.
One thing we quickly learned with four different faculty preceptors was each had different ideas of how to document. While it ultimately took several weeks into the clinic operation to agree and create templates for medical chart documentation, treatment plans and progress notes, students learned and practiced various methods of medical documentation and it spurred them to add an appendix to the policy and procedure manual of accepted medical abbreviations. For programs considering opening a clinic for students’ clinical educational experience, we strongly advise having clear and consistent directions with clinic operations and documentation prior to initiating patient visits.
Communication with patients regarding clinic policies, appointments and COVID-19-specific expectations is vital. To facilitate communication, scheduling and initiating care with patients, we created an email template and separate email account specifically for the clinic. The template and email account were used to communicate with patients and send them all required COVID-19 training, screening and welcome-to-campus items required by our university. To further encourage student involvement and management of the clinic, we assigned a student each week to monitor this email account who also scheduled new and returning patients.
Since a clinic needs patients to operate, we determined we would draw our initial patient population from faculty, staff and students associated with the athletic training program, expanding as needed to recruit friends and family. This allowed the clinic to have a slow rollout, while also providing immediate access to a variety of patient cases. Though a smaller patient case load consequently generated times without active patients in the clinic, it was during these times our second-year cohort students proactively facilitated peer-teaching moments with the first-year cohort. Often this included demonstrating and practicing skills, though it also fostered natural creation of guided simulated experiences encompassing scaffolding of knowledge, skills and abilities across a variety of domains to effectively manage complex patient care scenarios.
One benefit derived from creating the clinic was the peer assisted learning (PAL) that naturally occurred. From day one of the clinic opening and seeing patients, the second-year cohort students intuitively took on the role of teacher and mentor to the first-year cohort students that were assigned to the clinic as their clinical site. One student commented that the clinic “was a great opportunity to test my knowledge through teaching the first years.” Henning, Widener and Jones defined PAL in athletic training as a process of gaining knowledge, understanding or skill in athletic training-related tasks among students who are at either different or equivalent academic or experiential levels through instruction or experience.6 Athletic training education research concludes that students believed PAL improved confidence in psychomotor skills, increased communication skills and built strong relationships with peers.6,8 Moreover, PAL compels and promotes professional socialization, an important factor that can positively impact students’ diagnostic reasoning development and abilities.9
This clinic exposed students to varied experiences of professional socialization beyond faculty and preceptor mentorship, facilitating PAL interactions as an additional avenue for students to experience feedback during their ongoing clinical and professional development and transition to practice.9 While the faculty preceptors would check in, seek progress updates about patient cases and offer collaborative feedback during clinic time, in most cases the preceptors made little to none of the patient evaluation and treatment decisions. This further encouraged the students to work in pairs or small groups and collaboratively arrive at diagnosis and treatment recommendations.
Overall, the opening of our educational lab to serve as an athletic training experience for students was favorably received, and students, especially students in the second-year cohort, commented that it was one of their best clinical experiences. The students, sometimes for the first time, were able to see a patient from day one and autonomously create treatment and progress plans.
One student commented, “I really felt as if I were an independent practitioner making meaningful decisions that helped my patients.”
Students were presented with more complex cases (biceps tendon rupture, sacral dysfunction, headache-migraine clinical profile secondary to concussion, hip labral tear, serratus anterior strain) and a varied patient population, with one student commenting, “This experience was unique that allowed us to practice the skills we have learned. It provided a wide demographic that challenged our critical thinking and allowed us opportunities to grow and become more proficient athletic trainers.”
The faculty preceptors were able to spend extended time in conversations with students and often the entire clinic would learn and gain from patient cases other students were leading. At one point in the term, we encouraged students to hold a “grand rounds.” Two students each presented their complex patient cases to their peers, which were in the early phases of evaluation and treatment, and sought collaborative feedback and suggestions regarding diagnosis and treatment interventions. This dynamic peer-assisted diagnostic reasoning opportunity was another unexpected benefit of the clinic.
We made the decision to turn our teaching lab into an operating clinic during the pandemic to assist with the loss of athletic training clinical experience. What ultimately occurred were rich learning experiences encompassing direct patient care while providing varied opportunities and teachable moments for our students. Students proactively initiated PAL and gained valuable experience in administrative tasks prior to professional practice.
For programs investigating athletic training experiences and considering opening a clinic we recommend considering necessary approvals, medical direction and standing orders, documentation, clinical documents and forms, patient communication and daily operations policy and procedures.
Clinical education for athletic training students was suddenly questionable for some programs and came to a standstill for others when the COVID-19 pandemic began its first nationwide toll in the U.S. in March 2020. As such, athletic training programs were faced with the ongoing challenge of cultivating athletic training student skill development in preparation for professional practice. While supplemental clinical experiences such as simulation and/or telemedicine and telehealth were acceptable to meet educational requirements and on-time graduation1,3, athletic training programs remained obligated to teach and assess curricular content standards and require clinical education while preparing future athletic trainers to be safe and effective health care providers.
Clinical education and patient interaction are important parts of students’ education and many clinical education coordinators may be struggling to find or replace experiences that still challenge athletic training students similar to immediate care and participation in practices and events during the pandemic. For much of the U.S., fall 2020 continued to challenge programs’ ability to place students in clinical educational experiences.
As our clinical education team at Pacific University met to discuss moving forward with clinical education, we began to investigate alternative strategies that would enable students to utilize skills through direct patient-care opportunities, rather than only creating guided simulation experiences. As a solution, our program transitioned our teaching lab into an operating clinic during the COVID-19 pandemic to provide valuable hands-on athletic training experiences for students. For those programs looking to create patient care opportunities, figure 1 provides a list of key considerations.
During the current pandemic, programs must consider all necessary approvals to create a functional clinic on campus. These may be specific institutional COVID-19 tasks forces, college and school directors and deans and legal counsel. Consideration of financial costs, physical space, accessing patients, patient safety and any Centers for Disease Control and Prevention (CDC), state and/or regional mandates.
At Pacific University, our program is housed in the College of Health Professions, where several clinics already function. As such, we had successful models to follow and the process of approval was relatively quick.
Athletic trainers work under the direction of or in collaboration with a supervising physician. All accredited athletic training programs have a medical director, who can be a valuable advocate for creating a clinic and naturally fill the role of supervising physician. In developing our clinic, we worked with our medical director to enter into an agreement to serve as our supervisory physician and create standing orders. These standing orders emphasized musculoskeletal evaluation, treatment and rehabilitation to include electrical and manual therapies, supportive techniques, such as taping and bracing, functional testing and ongoing evaluation as deemed necessary and appropriate. University faculty would serve as preceptors. The emphasis on musculoskeletal conditions was purposeful since we would not see injuries associated with trauma or bleeding, therefore our standing orders did not include skills and procedures associated with emergency care.
Consideration of space and available equipment to evaluate and treat patients is important, especially when following CDC, state and/or regional guidelines for appropriate spacing needs for safe patient care. Our program has a dedicated teaching lab space of about 1,600-square-feet with 10 treatment tables, a treadmill, bike, various therapeutic modalities (e.g., ice packs, moist heat packs, paraffin, electrical stimulation and ultrasound, portable TENS units and cold pneumatic compression) and rehabilitation equipment (e.g., elastic bands, hand-held and cuff weights, foam rollers, BOSU balance pads, Theraballs, squat rack and weights). Our teaching lab space and the presence of equipment already used for educational purposes was ideal for transitioning into an active clinical site. While we had access to the equipment listed, opening an active clinic in teaching spaces can be successful with creativity and use of equipment you may already have available.
When discussing clinic hours of operation, we identified an afternoon schedule that would best fit our students' needs as classes would be complete by the afternoon.
As programs prepare future health care providers, one content area often cited as a weakness is administration.4,5 When developing a clinic, there are many policies and procedures, clinic documents and forms, and now COVID-19 screening protocols that must be created. Assigning these administrative tasks to students supports active practice and experience with creating and implementing administrative tasks that may not occur often during students’ traditional athletic training experiences. The students in our program had very little previous administrative experience, therefore it was a great opportunity for them to create new documents and templates and build a policy and procedure manual from the ground up. Our first-year cohort was actively involved in this administration piece as well, collaborating, reviewing and creating missing parts of the policy and procedure manual.
As a faculty, we served as preceptors and felt strongly about pushing students to take ownership of the clinic, thereby leaving a lot of the decision-making to them, which included mission and vision, patient confidentiality, code of conduct and professionalism, emergency action plan, and policies regarding clinic operations. This proved to be valuable, enabling them to feel ownership of and buy into the clinic, offering students an experience different from other clinical sites that may have followed a more hierarchical management style.
It is also important to consider electronic medical records (EMR) program and means of documentation when developing a clinic. When considering best documentation practices, also consider costs. Due to our program not having any funding for an EMR program, we elected to use paper documentation. While CAATE standards emphasize use of electronic health records to document health-related information, we found that returning to hand-written documentation further created teachable moments and underlined the importance of appropriate medical charting and documentation for our students.
One thing we quickly learned with four different faculty preceptors was each had different ideas of how to document. While it ultimately took several weeks into the clinic operation to agree and create templates for medical chart documentation, treatment plans and progress notes, students learned and practiced various methods of medical documentation and it spurred them to add an appendix to the policy and procedure manual of accepted medical abbreviations. For programs considering opening a clinic for students’ clinical educational experience, we strongly advise having clear and consistent directions with clinic operations and documentation prior to initiating patient visits.
Communication with patients regarding clinic policies, appointments and COVID-19-specific expectations is vital. To facilitate communication, scheduling and initiating care with patients, we created an email template and separate email account specifically for the clinic. The template and email account were used to communicate with patients and send them all required COVID-19 training, screening and welcome-to-campus items required by our university. To further encourage student involvement and management of the clinic, we assigned a student each week to monitor this email account who also scheduled new and returning patients.
Since a clinic needs patients to operate, we determined we would draw our initial patient population from faculty, staff and students associated with the athletic training program, expanding as needed to recruit friends and family. This allowed the clinic to have a slow rollout, while also providing immediate access to a variety of patient cases. Though a smaller patient case load consequently generated times without active patients in the clinic, it was during these times our second-year cohort students proactively facilitated peer-teaching moments with the first-year cohort. Often this included demonstrating and practicing skills, though it also fostered natural creation of guided simulated experiences encompassing scaffolding of knowledge, skills and abilities across a variety of domains to effectively manage complex patient care scenarios.
One benefit derived from creating the clinic was the peer assisted learning (PAL) that naturally occurred. From day one of the clinic opening and seeing patients, the second-year cohort students intuitively took on the role of teacher and mentor to the first-year cohort students that were assigned to the clinic as their clinical site. One student commented that the clinic “was a great opportunity to test my knowledge through teaching the first years.” Henning, Widener and Jones defined PAL in athletic training as a process of gaining knowledge, understanding or skill in athletic training-related tasks among students who are at either different or equivalent academic or experiential levels through instruction or experience.6 Athletic training education research concludes that students believed PAL improved confidence in psychomotor skills, increased communication skills and built strong relationships with peers.6,8 Moreover, PAL compels and promotes professional socialization, an important factor that can positively impact students’ diagnostic reasoning development and abilities.9
This clinic exposed students to varied experiences of professional socialization beyond faculty and preceptor mentorship, facilitating PAL interactions as an additional avenue for students to experience feedback during their ongoing clinical and professional development and transition to practice.9 While the faculty preceptors would check in, seek progress updates about patient cases and offer collaborative feedback during clinic time, in most cases the preceptors made little to none of the patient evaluation and treatment decisions. This further encouraged the students to work in pairs or small groups and collaboratively arrive at diagnosis and treatment recommendations.
Overall, the opening of our educational lab to serve as an athletic training experience for students was favorably received, and students, especially students in the second-year cohort, commented that it was one of their best clinical experiences. The students, sometimes for the first time, were able to see a patient from day one and autonomously create treatment and progress plans.
One student commented, “I really felt as if I were an independent practitioner making meaningful decisions that helped my patients.”
Students were presented with more complex cases (biceps tendon rupture, sacral dysfunction, headache-migraine clinical profile secondary to concussion, hip labral tear, serratus anterior strain) and a varied patient population, with one student commenting, “This experience was unique that allowed us to practice the skills we have learned. It provided a wide demographic that challenged our critical thinking and allowed us opportunities to grow and become more proficient athletic trainers.”
The faculty preceptors were able to spend extended time in conversations with students and often the entire clinic would learn and gain from patient cases other students were leading. At one point in the term, we encouraged students to hold a “grand rounds.” Two students each presented their complex patient cases to their peers, which were in the early phases of evaluation and treatment, and sought collaborative feedback and suggestions regarding diagnosis and treatment interventions. This dynamic peer-assisted diagnostic reasoning opportunity was another unexpected benefit of the clinic.
We made the decision to turn our teaching lab into an operating clinic during the pandemic to assist with the loss of athletic training clinical experience. What ultimately occurred were rich learning experiences encompassing direct patient care while providing varied opportunities and teachable moments for our students. Students proactively initiated PAL and gained valuable experience in administrative tasks prior to professional practice.
For programs investigating athletic training experiences and considering opening a clinic we recommend considering necessary approvals, medical direction and standing orders, documentation, clinical documents and forms, patient communication and daily operations policy and procedures.
References
1. CAATE Statement on Coronavirus on the Delivery of Clinical Education. CAATE.net.
https://caate.net/wp-content/uploads/2020/03/CAATE-Update-on-Coronavirus... Published March 11, 2020. Accessed December, 15, 2020
2. CAATE Update on the Coronavirus. CAATE.net. https://caate.net/wp-content/uploads/2020/03/3.13.20-CAATE-Coronavirus-U.... Published March 19, 2020. Accessed December, 15, 2020
3. Implementation and Guide to the CAATE 2020 Professional Standards. CAATE.net. https://caate.net/wp-content/uploads/2020/11/Pursuing-and-Maintaining-Ac.... Published January 9, 2018. Accessed December 8, 2020.
4. Carr WD, Volberding J. Employer and employee opinions of thematic deficiencies in new athletic training graduations. Athl Train Educ J. 2012;7(2):53-59.
5. Mazerolle SM, Whitney M, Eason C. Examining the experiences of athletic trainers as they transition into their full-time position. J Sports Med Allied Health. 2017;2(3):1-18.
6. Henning JM, Weidner TG, Jones J. Peer-assisted learning in the athletic training clinical setting. J Athl Train. 2006;41(1):102–108.
7. Bates DK. Perceptions from graduates of professional athletic training programs involved in peer-assisted learning. Athl Train Educ J. 2014;9(3):113–126.
8. Mackey T, Kamphoff C, Armstrong J. Perceptions of participants involved in peer assisted learning in a professional athletic training education program. Athl Train Educ J. 2010;5(1):13–20.
9. Kicklighter TH, Geisler PR, Barnum M, Heinerichs S, Martin M. (2018). Exploration of factors perceived to influence development of diagnostic reasoning in athletic trainers and athletic training students. Athl Train Educ J. 2018;13(2),120-130.




